Stop Squatting Through That Painful Hip Pinch!



There’s No Excuse To Squat Through Hip Pain
You heard me! Stop squatting through that “tightness”, “pinching sensation” in the front of your hip. Many times, people say that they feel a “pinching” or “tight” feeling on the front of their hip when they squat. Most of the time, it is felt as they approach parallel.
There are many reasons why that hip “pinch” may be present. They can include:
- Decrease Joint Capsule Mobility
- Decrease Soft Tissue Mobility
- Pelvic/Hip Bone Structure
- Poor Technique
Since we know that everyone presents with unique body structure and have individualized needs as I highlighted in my article “Why People Need To Deadlift Differently” let’s start off looking at the major causes of hip pinching in the squat.
1. Limited Joint Capsule Mobility
Some people can present with a decrease in the mobility of the hip joint capsule. The hip joint capsule is synonymous to a Zip-loc bag that surrounds the joint. When the hip is placed into varying positions, certain aspects of the capsule can become “taut.”
In regards to squatting, the posterior and inferior aspect of the capsule can become taut. When this occurs, the point on which the femoral head rotates can translate anteriorly and alter the biomechanics of the hip joint. In turn, this can cause a pinch in the front of the hip.
In my experience as a clinician and coach, this is one of the lesser common reasons why someone may experience pinching when squatting, but one that many people gravitate towards in self-diagnosis.
If you truly present with joint capsule mobility deficits, seeking out a qualified manual therapy physical therapist of rehab pro should be your next step. But like I mentioned, a vast majority of people will fall into the next three major categories of causation for hip pinching in the squat so do yourself a favor and explore all the self-sufficient options first.
2. Limited Soft Tissue Mobility
Muscles that cross a joint can have increased “tightness or tone” and can limit mobility at joints throughout the body. The same can be said for the hip.
These various muscles can limit movements in all directions associated with the hip. These muscles can include:
- Gluteus Maximus
- Adductors (the ones that extend the hip)
- Rectus Femoris/Vastus Lateralis
- Iliacus
- Tensor Fasciae Latae (TFL)
- Hip External/Internal Rotators
The gluteus maximus can limit hip flexion because of its role as a hip extender. The adductors that extend the hip can also limit hip flexion similar to how the glutes do. External and internal rotators of the hip aren’t a major player in limiting hip flexion, but they can play a role in some cases due to their attachments on the pelvis and femur.
Now, when it comes to Rectus Femoris, Vastus Lateralis, Iliacus, and Tensor Fascia Latae, how can muscles that “flex hip hip” or variations there of limit hip flexion. Technically, shouldn’t these muscles be on slack during a hip flexion moment?
What we need to consider is the orientation of these muscles and their attachment points. In standing, if there is increased tone and tightness in the aforementioned muscles, they can place the hip/pelvis into an anterior rotated position. Neuman 2010.
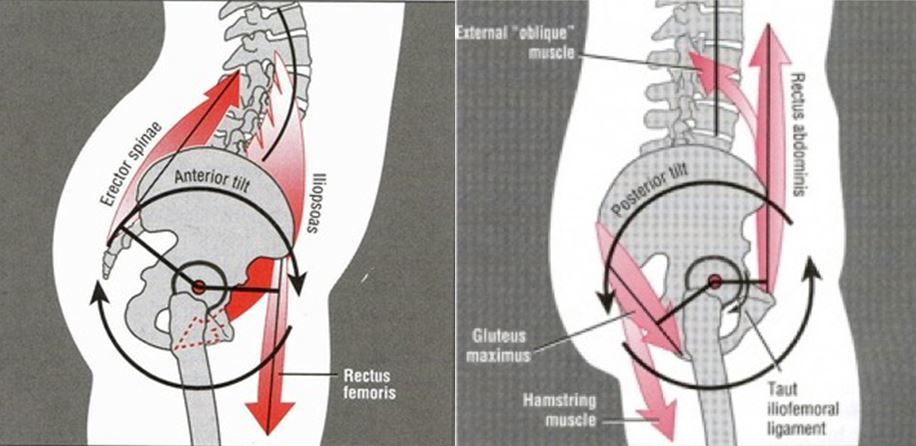
In turn, due to this anterior pelvic tilt, it will decrease the amount of space necessary to allow for the hip to flex because of the decreased amount of space between the acetabulum and the femoral head.
To determine if someone has decreased hip extension mobility or increased tone in the “hip flexor musculature,” try performing the Thomas Test.
If you are not a clinician or a coach but want to put yourself through some hip flexor testing to determine soft tissue involvement, check out this self Thomas Test below:
When performing this test on yourself, you are looking to see if:
- Thigh can become perpendicular to the table.
- Knee at 90 degrees.
- Thigh is NOT abducting out to the side.
If you are performing this on someone else, you are going to palpate the Anterior Superior Iliac Spine (ASIS). This is the hip bone on the front of the body where your quadriceps attaches on.
As you lower the leg, you are feeling for anterior translation of the ASIS into your thumb. If you can lower the leg without feeling anterior translation, then you have normal hip flexor mobility.
If you feel it translate prior to reaching the table, you can tease out which muscle group could be limiting hip extension mobility. Here’s how to differentiate the findings of the Thomas Test:
- By straightening the knee, if the thigh descends to the table normally, then Rectus Femoris is to blame.
- By straightening the knee, if the thigh descends towards the table and the ASIS still translates anteriorly, then Iliacus/Psoas is the most likely culprit.
- If you abduct the thigh and the thigh descends normally, then you know TFL is NOT the likely cause of immobility.
- If it translates, then TFL is to blame. If you perform the test with the knee flexed and hip abducted and the ASIS does translate anteriorly, then Vastus Lateralis is to blame.
If any of those tests came back positive, try performing some type of Self-Myofascial Release (SMR) to help improve that mobility. Start by addressing the Iliacus, Psoas and Tensor Fascia Lata with the foam rolling technique below:
If there is more of a need to address the big muscles of the quadriceps and “IT-Band tightness” then you can move on to using the Vastus Lateralis and Tensor Fascia Lata foam rolling techniques showcased in the video below:
But here, the deal… Anytime you use a technique to remediate mobility or movement, we must test and re-test. So, re-test it to see if it has improved. If so, great! If not, seek out a physical therapist, sports chiropractor, massage therapist, etc.
It should be mentioned as well that along with direct soft tissue work for these muscles, we can also “unlock” mobility with more active based corrective strategies like the ones I highlighted in “The Top 5 Most Effective Hip Mobility Drills”.
3. Pelvic & Hip Structure
Barring any unforeseen circumstances, the majority of people are born with two femurs and two acetabuli aka the socket of the hip. But remember, people’s anatomy are NOT all created equally. What this means is that femur and acetabulum position can vary from person to person and side to side in the same person.
Check out these pictures courtesy of our friend Dr. Ryan DeBell of The Movement Fix:
These are some amazing pictures are of shape and orientation of the pelvis and femurs. The first picture shows the varying angles that the femur can present at.
 Some people present like the one on the left while others present like the one on the right. People also can be in between these two variations. This bony position will partly determine how someone’s foot position will be when squatting. Some people can squat with their feet straight ahead while others may need to turn their feet outwards.
Some people present like the one on the left while others present like the one on the right. People also can be in between these two variations. This bony position will partly determine how someone’s foot position will be when squatting. Some people can squat with their feet straight ahead while others may need to turn their feet outwards.
The next picture shows the angle or position of the acetabulum (hip socket).

Pelvis #1 (left) will most likely need to “toe out” slightly as compared to pelvis #2 (right) that may be able to squat will less difficulty with their feet pointing straight ahead. This is due to the orientation of their hip sockets and how their femurs will orientate themselves.
This goes to show that some people cannot perform the squat with their feet straight ahead or shoulder width apart. Some people need to adjust to go a little bit wider, toe out more, etc. The only way to change the position of your femurs or acetabuli is surgically.
And before you ask it, NO! With bony anatomical variations that limit specific squat setups and patterns, you cannot “out-stretch” it, so don’t even try as I’ve highlighted in the article “Why Your Hamstring Stretching Habit Is A Hoax”. This is another reason why if you are squatting, you may be experiencing a hip pinch.
For more reading on the specifics of anatomical hip joint structure, make sure to check out Ryan DeBell’s great article, “Why People Have to Squat Differently”.
4. Poor Technique
Lastly and most importantly, technique can play a major role in how proficient you can be when squatting. One can exhibit pristine technique and be able to perform an “Ass to Grass” squat while others perform a squat with atrocious technique, “butt wink,” and increase their risk for injury.
In regards to the “hip pinch” and the role that technique plays, check out this picture:

If you start your squat or perform your squat with a large “arch” or in excessive extension at your lumbar spine, eventually one of three things will happen.
- You won’t be able to squat as deep as you would like.
- “Butt Wink” where the spine will go from lumbar extension to neutral spine and into lumbar flexion, all while under load.
- “Hip Pinch” as you descent into the squat.
Instead, try performing your squat starting in a more “neutral position.”
As you can see in the video, the lifter slightly “tucks his tailbone,” or go from slight extension into a more neutral spine alignment. By doing this, the lifter can descend into the squat, maintain a neutral spine, attain proper depth, and not experience a hip pain.
By starting in extension, this relates back to the part of this post about anterior pelvic tilt. Eventually, the lifter will run out of space at the hip and will either not be able to squat to depth, “butt wink,” or feel a pinch in the front of their hip.
This is the first place to start when looking to rid your squats of pinching hip pain. Perfect your technique and determine what squat variation best fits your body. To get started with this process, refer to Dr. Michael Mash‘s articles, “Which Barbell Squat Variation Is Optimal For You” and “Hip Pain While Squatting” to lock down your setup and squat type with confidence.
Stop squatting through that hip pinch! Check our joint and soft tissue mobility, adjust your technique based off the type of hip you may present with, and dial in your technique to avoid that hip pinch!
About The Author
Related Posts





7 Comments
Leave A Comment

Hello,
I am not sure if you will answer questions here in comments but I thought to give it a try.
I did the Thomas test and I felt the same “pinch” or tightness in my hip (I guess it is iliacus or psoas major) as sometimes when I am squatting. This pinch was only on left side. This is more common with back squat than front squat. Because this is more in the other side I guess it would be tightness on the other side. Can you help to identify the problem?
Thanks,
Sami
Hi Sami,
Thank you for reading the article! Difficult to determine online. My best suggestion would be to get assessed by a physical therapist in your area. Where are you located?
Best,
Andre
Yet another article suggesting that all pain can be overcome with training right or rehabilitation exercises…Yes true for most people, but not for me with totally destroyed labrums due to an old trauma being largely responsible for my hip pain. Beware physical therapists telling you to do tons of ‘corrective’ exercises without even ordering imaging of the join that is hurting.
Hi Alison,
Thank you for reading the article. Not all pain can be overcome with training right/rehab exercises, but it can help quite a bit. As with most things, if someone is still experiencing pain, get checked out by a sports chiropractor, physical therapist, etc.
Imaging doesn’t tell the whole story. Based off a thorough movement assessment and a focused plan, people can move well and pain free even with imaging that may say otherwise. Yes, there are rehab professionals giving out too many corrective exercises. The right corrective exercise combined with an individualized strength and conditioning program can make all the difference.
Please can you clarify a point for me:
When doing the Thomas’ test – Once in position your point 3 says ‘ if you abduct the thigh and the thigh descends normally, then you know TFL is NOT the likely cause of immobility.’
Is abducting the thigh not taking the ITB and hence TFL off stretch – so if they were tight the thigh descending at this point in the test WOULD suggest that the TFL is the culprit? Maybe i am getting confused and this just apply to ITB and not TFL???? – I have always done this test for ITB.
Thanks
I would like to hear the answer to this as well. That part did not made sense to me, especially the way it is written. There is tons of Thomas Test info elsewhere though.
Hello, what would you recommend to someone who has a torn labrum in one hip. X-ray also showed that the lateral neck of my right femur is “flat.” I have always had trouble squatting, and once diagnosed, it made sense. However no one really gave me instructions on how to work around it. They just said if it hurts, stop.